

Endovascular treatment of an aortoiliac aneurysm with concomitant left pelvic kidney and ectopic origin of the renal artery

| Available Online: | September, 2023 |
| Page: | 108-111 |
Author for correspondence:
Senka Sprem
Protestant Hospital of Bergisch Gladbach (EVK) Ferrenbergstraße 24, 51465 Bergisch Gladbach – Germany
E-mail: senka.sprem@gmail.com
doi: 10.59037/hjves.v5i3.42
ISSN 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications
All rights reserved. https://www.heljves.com
Abstract
Full Text
References
Image
Abstract
Abstract:
Purpose: An aortoiliac aneurysm with a pelvic kidney is a quite rare coincidence. The general challenge of open surgery treatment of such a condition is to avoid prolonged intervals of renal ischemia with possible impairment of renal function. In recent times endovascular treatments also are performed, as these only include minimal ischemic phases, mainly due to inflated modelling balloons.
Case report: We present a case report describing the successful endovascular treatment of a 66-year-old patient with an aortoiliac aneurysm and a concomitant left pelvic kidney using a single-branched endoprosthesis and an iliac side branch with the corresponding prosthesis extensions and covered stents.
Conclusion: We highlight in this case report that the deployment of a custom-made device for the treatment of an aorto-il- iac aneurysm with renal anomaly is a feasible solution. However, a strict follow-up is necessary up to long term.
Full Text
INTRODUCTION
Preservation of the main arteries originating from the aorta is one of the many challenges in the surgical treatment of aortic diseases. This applies to the aortic arch as well as the visceral and infrarenal aortic segments IV. and V., in open surgery and endovascular procedures. In addition, the continuous development of endovascular techniques increasingly enables the treatment of atypical and more complex anatomical findings. Here we present a case of successfully endovascular treated aortic pathology while preserving a patent artery to an ectopic kidney.
CASE REPORT
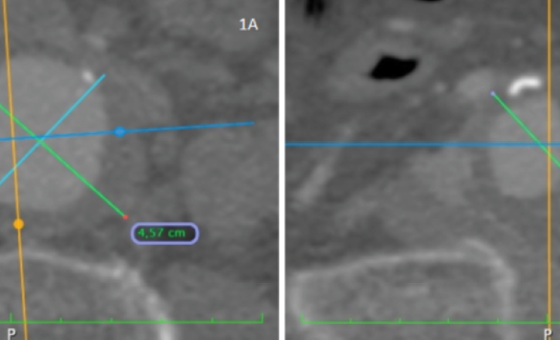
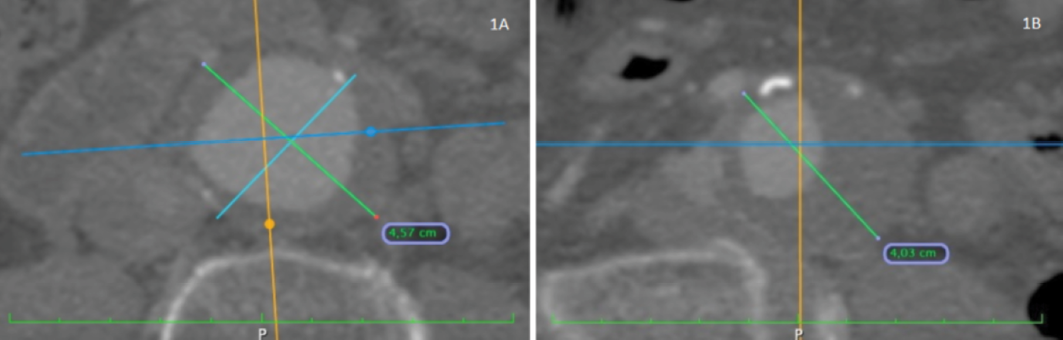
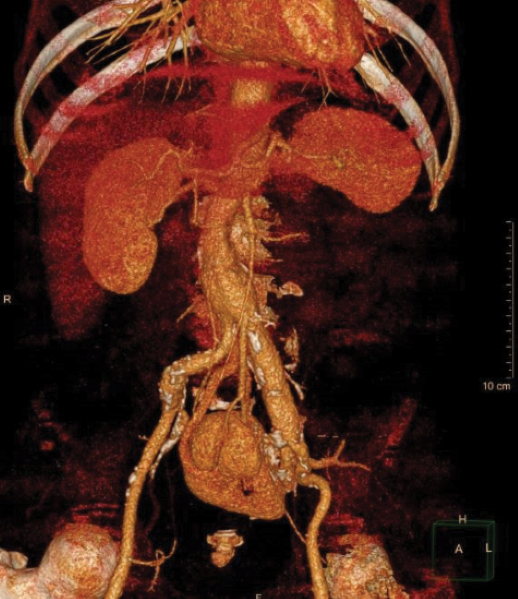
A 66-year-old patient was admitted to our hospital with an incidental sonographic finding of an infrarenal aortic aneurysm. This finding is accompanied by coronary heart disease (state after a cardiac infarction) and hyperthyroidism as comorbidities of the patient. Computed tomography angiography (CTA) performed for preoperative planning confirmed the presence of an infrarenal aneurysm involving the left common iliac artery and iliac bifurcation, with a maximum diameter of the infrarenal aortic aneurysm of 45,7 mm and a maximum diameter of the common iliac artery of 40,3 mm (Figures 1a and 1b). As a further incidental finding, we identified a left pelvic kidney supplied by a renal artery atypically originating from the left common iliac artery, directly distal to the aortic bifurcation (Figure 2)
Thus, the surgical treatment required the exclusion of the aortoiliac aneurysm while preserving perfusion of the left internal iliac artery and the atypical left renal artery. We have performed the implantation of a custom-made device whose customization has lasted 3 weeks.
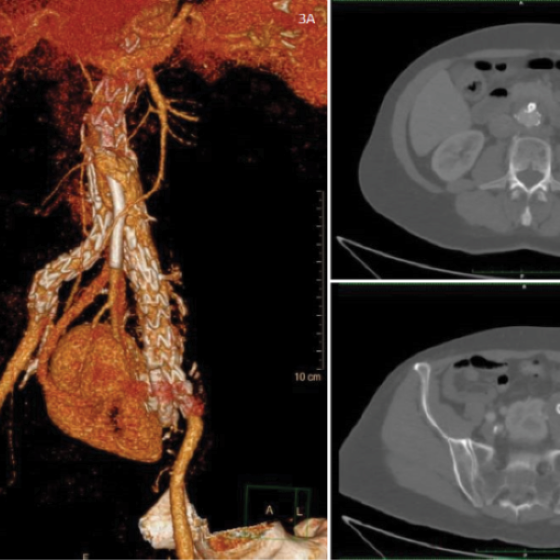
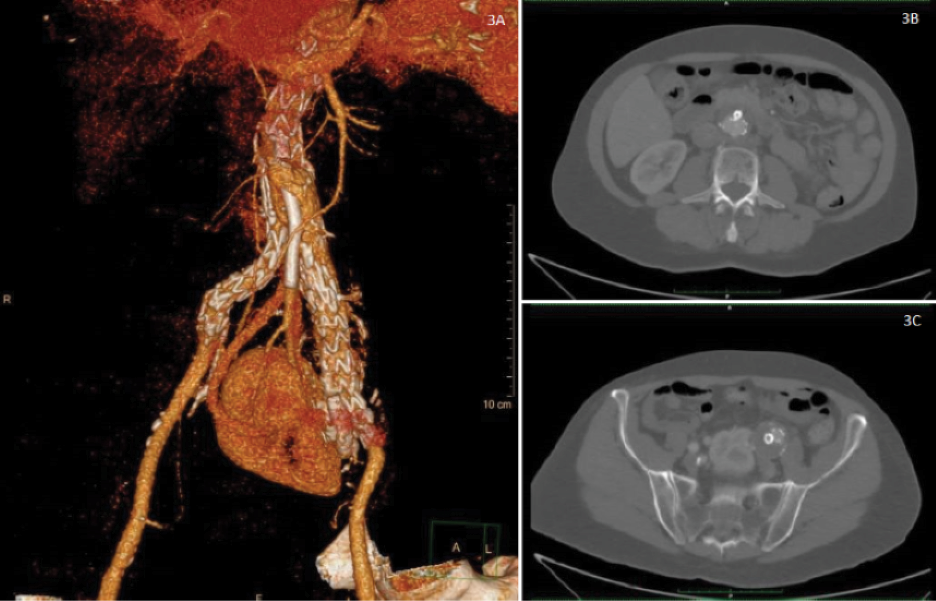
The procedure was performed under general anaesthesia with vascular access via the left and right femoral artery and left subclavian artery. A single-branched Jotec E-Tegra endoprosthesis and a Jotec E-liac iliac side branch with the corresponding prosthesis extensions and covered stents were used. The whole procedure lasted 3 hours and 47minutes. Intraoperative angiography documented a complete exclusion of the aortoiliac aneurysm from blood circulation without any persisting endoleaks and this was confirmed by a post-operative CT angiography (Figures 3a, 3b and 3c).
The patient was monitored on the intensive care unit for one night and transferred back to the peripheral ward afterwards. We were able to discharge the patient on the third day after surgery. Parameters for renal function were monitored daily and showed no elevation above the normal range. CT angiography on the day of discharge documented a perfect positioning of all prosthetic components. As follow-up, at first a CT angiography after 6 months was planned, and regular ultra-sound control recommended.
DISCUSSION
A pelvic kidney occurs when an error takes place during the ascent of the kidney in the early development stages, leading the kidney to remain in the pelvis, instead of the abdomen1.
The vasculature of the pelvic kidney has been reported as complicated and highly variable, which is due to the pelvic kidney retaining its foetal blood supply2. The incidence of a pelvic kidney is given as 1 in 2000 up to 1 in 3000 3. The incidence of an abdominal aortic aneurysm is 1 in 300 to 1 in 10004, the incidence of aortoiliac aneurysms is even less. The combined frequency for the coincidence of both pathologies might be approximated as 1 in 600000 to 1 in 3000000. The coincidence of an aortoiliac aneurysm with a pelvic kidney thus is quite rare.
In 2003, a radiologic survey of 1650 patients undergoing infrarenal aortic surgery found three individuals with a pelvic kidney5. A literature search accompanying a published case in 2018, including scientific papers from 1977 onwards to 2015, found 27 cases of an abdominal aortic aneurysm associated with a pelvic kidney; of these patients, 22 received open surgery, hybrid procedures were performed in 2, and total endovascular repair in 3 cases6. At least one case since then was published utilizing the chimney technique7.
In open surgery, a concomitant pelvic kidney with an ectopic origin of its renal artery also requires the renal artery’s excision out of the aortic wall and reinsertion into the prosthesis while avoiding prolonged intervals of renal ischemia with possible impairment of renal function. An ischemic phase of 30 up to 40 minutes is usually thought to be tolerable. However, if the expected ischemic phase is longer, temporary renal bypass or shunting procedures8,9 or protective renal perfusion with hypothermic solutions10 are recommended.
Open surgical procedures have been increasingly superseded by endovascular aortic repair (EVAR) during the past decades. Apart from greater patient comfort, cross-clamping phases of the aorta or visceral arteries can be avoided, and only minimal ischemic phases, e. g. due to inflated modelling balloons are necessary. Thus, EVAR procedures seem to provide significant benefits in minimizing potential ischemic damage to the kidney and other abdominal viscera. In the presented case, the extensive coronary artery disease as comorbidity, the expected longer cross-clamping phase due to the complex vascular anatomy in an open surgery, and the patient’s wish were significant arguments for performing the described procedure. However, case studies and other scientific work on that topic are still rare.
CONCLUSION
We here report the successful endovascular treatment of a 66-year-old patient with an aortoiliac aneurysm and a concomitant left pelvic kidney. The deployment of a custom-made device for the treatment of an aorto-iliac aneurysm with renal anomaly is a feasible solution. However, strict follow-up is necessary up to long term.
References
-
REFERENCES
- Eid S, Iwanaga J, Loukas M, et al. Pelvic Kidney: A Re- view of the Literature. Cureus 10(6), https://dx.doi. org/10.7759%2Fcureus.2775
- Dretler SP, Olsson C, Pfister RC. The anatomic, radiologic and clinical characteristics of the pelvic kidney: an anal- ysis of 86 cases. J Urol. 1971;105(5):623-7. https://doi. org/10.1016/S0022-5347(17)61591-X
- Stevens AR. Pelvic Single Kidneys. J Urol. 1937;37(5):610- 8. https://doi.org/10.1016/S0022-5347(17)72061-7
- Zommorodi S, Leander K, Roy J, Steuer J, Hultgren R. Understanding abdominal aortic aneurysm epide- miology: socioeconomic position affects outcome. J Epidemiol Community Health. 2018;72(10):904-10. https://doi.org/10.1136/jech-2018-210644
- Faggioli G, Freyrie A, Pilato A, Ferri M, Curti T, Paragona O, u. a. Renal anomalies in aortic surgery: Contemporary re- sults. Surg. 2003;133(6):641-6. https://doi.org/10.1067/ msy.2003.15
- Bianchini Massoni C, Azzarone M, Barbarisi D, Perini P, Frey- rie A. Ruptured Abdominal Aortic Aneurysm in a Patient with Congenital Fused Pelvic Kidney: A Case Report of Emer- gency Endovascular Treatment. Aorta. 2018;06(01):021-7. https://doi.org/10.1055/s-0038-1636992
- Ertugay S, Posacioglu H, Bozkaya H, Parildar M. Chimney technique for solitary pelvic kidney. Interact Cardiovasc Thorac Surg. 2020;31(5):743-4. https://doi.org/10.1093/ icvts/ivaa154
- Makris SA, Kanellopoulos E, Chronopoulos A, Vrachliotis TG, Doundoulakis N. A double shunt technique for the prevention of ischaemia of a congenital, solitary, pelvic kidney during abdominal aortic aneurysm repair: a case report. J Med Case Reports. 2011;5(1):92. https://doi. org/10.1186/1752-1947-5-92
- Malinowski MJ, Al-Nouri O, Hershberger R, Halandras PM, Aulivola B, Cho JS. Abdominal Aortic Aneurysm As- sociated with Congenital Solitary Pelvic Kidney Treated with Novel Hybrid Technique. Ann Vasc Surg. 2014;28(6). https://doi.org/10.1016/j.avsg.2014.01.015
- Faggioli G, Freyrie A, Pilato A, Ferri M, Curti T, Paragona O, et al. Renal anomalies in aortic surgery: Contemporary re- sults. Surg. 2003;133(6):641-6. https://doi.org/10.1067/ msy.2003.156

{kind=link}
{kind=link}
{kind=link}