

Outpatient treatment of truncal veins insufficiency

| Available Online: | September, 2023 |
| Page: | 45 -51 |
Author for correspondence:
Petros K. Chatzigakis
Department of Vascular Surgery, “G. GENNIMATAS” Athens
General Hospital. Mesogeion 154, 15669. Athens, Greece
Email: petros.chatzigakis@gmail.com
doi: 10.59037/hjves.v5i2.45
ISSN: 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery
Published by Rotonda Publications
All rights reserved. https://www.heljves.com
Petros K. Chatzigakis, Aikaterini Karolina Zianika, Georgios Geropapas, Alexios Kalamaras, Vasileios Katsikas, Georgios C. Kopadis
Department of Vascular Surgery “G. Gennimatas” Athens General Hospital
Abstract
Full Text
References
Images
Abstract
Abstract
Introduction: Chronic venous disease is a common clinical problem with an increasing incidence that constitutes a financial burden for healthcare. Minimal invasive techniques and procedures in an outpatient basis may help decompressing the healthcare system. The aim of this study is to evaluate the effectiveness and safety of endovenous closure of the truncal veins with n butylcyanoacrylate adhesive on an outpatient basis.
Methods: We treated 100 cases of venous insufficiency with endovenous NBCA glue closure of the truncal veins on an outpatient basis. Patients were usually admitted to the vascular surgery department at the time of the procedure. The surgery took place in the general operation room, under local anesthesia. We didn’t use compression stockings and patients were instructed to walk immediately after the operation.
Results: There was a 100% successful obliteration of the target vein in day 0, 2weeks, 3-months and one year. The majority of patients (98%) reported improvement of the symptoms, whereas 60 patients (60%) had complete elimination of symptoms. The appearance of varicose veins improved in 96% of the cases. There were no major adverse effects observed during follow-up. A percentage of 28% presented erythema and tenderness along GSV and 15 of those patients were treated with anti-inflammatory drugs (Ibuprofen) and 5 with antibiotics (Amoxicillin-Clavulanic acid).
Conclusion: Outpatient treatment of venous insufficiency with endovenous glue closure is a safe and efficient method. It increases patient satisfaction, permits rapid return to normal activities and reduces the risk of hospital transmission of infectious diseases and hospitalization costs.
Full Text
INTRODUCTION
Chronic venous disease (CVD) is one of the most common clinical problems, where chronic lower limb superficial venous disease affects approximately 35% of adults1. It is responsible for substantial morbidity as 1% to 4% presents serious complications at more advanced stages with a healed or active venous ulcer2,3,4. Limb heaviness, aching, soreness, fatigue, burning, oedema, and pigmentation are usual troublesome signs and symptoms of the disease 5,6,7.
The prevalence of CVD is very high and affects many millions of persons worldwide and incurs high costs for treatment. The incidence of CVD is almost 1 in 1000 persons per year, that meaning at least 150,000 new cases in the United States annually. In Western countries it consumes up to 2% of healthcare budgets 8. The chronic character of CVD and its high prevalence affect the lifestyle of many people. As a result, CVD must be seen as an important health, economic and social problem
Even more, CVD is a condition that tends to worsen with age, while western population is aging constantly and rapidly. As a result, the prevalence of CVD is projected to increase substantially, and the need to treat CVD patients will induce large increases in the healthcare resources and costs8.
The rationale of venous disease treatment is to decrease ambulatory venous hypertension. Traditional surgical techniques, with stripping, high ligation of the great saphenous vein (GSV), and avulsion of varices, involve significant discomfort and require anaesthesia and hospitalization. The newer minimally invasive vein surgery procedures even though require only local anaesthesia and are considered as one day procedures, they are still performed in most centers with a few hours’ hospitalization9.
In this study, we report our experience of superficial vein insufficiency treatment in an outpatient basis. The aim of the current study was to evaluate the treatment of superficial vein insufficiency in a totally outpatient basis, as far as effective- ness (anatomical success and clinical outcomes) and safety is concerned.
PATIENTS AND METHODS
Patients
The study was a purely retrospective review of the record. We present the results of 100 cases in 96 patients treated with endovenous embolization of truncal veins with NBCA, during the period between November 2019 and December 2021 in an outpatient setting. The procedure was performed under local anesthesia, did not require overnight stay and all patients were discharged within one hour from the operation. We used the VenaSeal Closure SystemTM (Medtronic Plc, Dublin, Ireland) with slowly polymerizing, high viscosity cyanoacrylate glue. All patients signed a consent form before entering the study. Only patients who had completed their follow-up were selected. The study included 61 women (63.5%) and 35 men (36.4%) with a mean age of 53 years (range 27-87). All patients had symptomatic GSV or SSV insufficiency. Patients were evaluated preoperatively with clinical examination and were classified according to 2004 CEAP (Clinical, Etiological, Anatomical and Pathophysiological) classification and the revised Venous Clinical Severity Score (rVCSS)10. They were examined with a deep and superficial vein duplex ultrasound with the patient both in supine and upright positioning, which was conducted by an independent certified radiologist. All patients were also subjected to a second duplex ultrasound, performed by the lead author, using a General Electric LOGIQ V2 (General Electric Healthcare) prior to any decision making.
Study eligibility inclusion criteria were: age over 18 years, ability to give informed consent, CEAP C2-C6, symptomatic venous insufficiency with reflux > 0.5sec on color Duplex and symptoms including heaviness, fatigue, soreness, burning, pruritus, discomfort and edema.
We evaluated our results by means of effectiveness and safety. Effectiveness includes anatomical and clinical success. Anatomical success as indicated by GSV occlusion rate on ultrasound examinations, is defined as no segments of patency longer than 3 cm and clinical success is assessed by the quality of life (QoL) using the revised Venous Clinical Severity Score. Regarding safety, all complications during and after the opera- tion and all adverse events were documented.
Postoperative evaluation was conducted at 2 weeks, 3 months and one year. Follow up included clinical examination and repetition of the rVCSS, as well as duplex ultrasound to ensure successful target vein closure and exclude the presence of deep vein thrombosis.
Methods and Procedural protocols
Patients were usually admitted to the vascular surgery department at the time of the procedure. The surgery took place in the general operation room, under local anesthesia. We used the Vena Seal Closure SystemTM (Medtronic Plc, Dublin, Ireland). The GSV is accessed at the distal point of reflux percutaneously with direct puncture or with a micropuncture introducer kit. When this approach is not feasible, a small incision (3mm) is made to facilitate open access to the vein. Usually this distal point is just above the medial malleolus, but it can be in every point along the saphenous vein path. The IFU of Vena Seal Closure SystemTM were followed for vein occlusion through glue delivery. When finished, the catheter is removed; compression is applied to the catheter entry site, as well as sutures in case of cut-down. Successful occlusion of the entire treated vein was confirmed by on-table duplex ultrasound.
Patients left the operating table walking. They were instructed to walk mildly and stay in the hospital for 45 minutes before being evaluated and then discharged. There was no post-operative use of bandages or compression stockings. They were encouraged to walk and were instructed to resume normal activities within a day. Postoperative ultrasound examination was performed immediately after surgery, at 15 days, three months and one year.
RESULTS
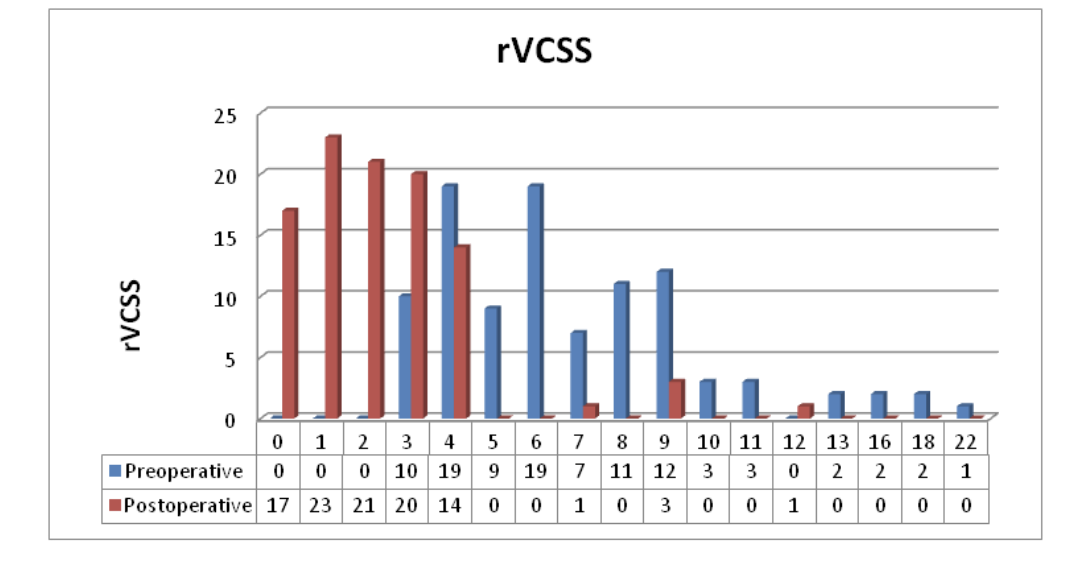
Patients’ CEAP classification was between C2 and C6. More specifically, 39 patients had varicose veins C2 (39%), 41 pa- tients were in stage C3 (41%) with venous edema, 15 patients in C4a (15%) presenting pigmentation or venous eczema, 2 patients in C5 (2%) with healed venous ulcer and 3 in C6 (3%) with active venous ulcer. (Table 1) The mean preoperative rVCSS was 6.8. Specifically, the VCSS for this cohort of patients is depicted analytically on table 2.
All patients underwent local anesthesia. In 63 patients (63%) there was a percutaneous approach via direct puncture, (10 patients needed a double puncture and one needed three punctures). A short 3 mm cut-down to expose the target vein was performed in 37 patients (37%). The access point was near the medial malleolus in 57 cases (57%), below the knee in 19 cases (19%), at the thigh in 10 cases (10%), while in three cases (3%) the SSV was the target vein. Five cases (5%) presented double GSV. All patients underwent an on-table completion ultrasound to verify successful ablation closure of the treated venous segment and to inspect the common femoral vein for deep venous thrombosis via compressibility test. There was a 100% successful obliteration of the target vein in day 0, 2weeks, 3-month and one year follow up
The vast majority of patients (98%) reported improvement of the symptoms, whereas 60 (60%) had complete elimination of symptoms. The appearance of varicose veins improved in 96% of the cases. Thirty-three patients (33%) presented complete obliteration of varicose veins, while 63% showed significant improvement of the appearance of varicose veins. All patients with an active venous ulcer (3) presented improvement of the ulcer within 2 weeks of the procedure and total healing in 3 months. All patients improved their rVCSS. Postoperative rVCSS was 2.3 with a mean 66% decrease (mean preoperative rVCSS was 6.8). (Table 3)
There were no major adverse effects observed during follow-up (pulmonary embolism, skin necrosis, TIA, nerve injury, infection). A percentage of 28% (28 patients) presented erythema and tenderness along GSV which was observed between second and seventh post-operative day, lasting approx- imately one week and gradually getting better. Of those who presented erythema the majority had a superficially placed GSV, out of the saphenous compartment, with very limited distance from the skin. Fifteen of those patients (15%) were treated with anti-inflammatory drugs (Ibuprofen) and five (5%) with antibiotics (Amoxicillin-Clavulanic acid). In 3 cases (3%) there was postoperative skin hyperpigmentation and in one case (1%) there was a superficial stitch abscess.
DISCUSSION
The treatment of CVD in the medical literature goes back since the time of Hippocrates11,12 and although since that time the treatment of CVD has evolved the standard open operation with high ligation and stripping of the GSV remained for many years the gold standard.
In modern medicine there is a trend towards less invasive and thus more comfortable for the patient and probably safer treatments, together with at least equal or even better re- sults. Chronic venous disease is not an exception to that, so the concept of minimally invasive procedures becomes in our days the new gold standard in vein surgery.
During the mid-20th century Robert Muller presented a technique using hook dissectors and multiple small skin inci- sions to treat superficial varices in an ambulatory way 13,14. He named his technique “ambulatory phlebectomy” and brought the first ambulatory treatment of superficial venous insufficiency into the modern world as we know today 15,16
Although this was an improvement, the real changes occurred during the last two decades with the appearance of the endovenous techniques. Open surgery methods, such as ligation and stripping, are associated with more complications, including hematoma and paraesthesia, with long recovery times and are considered risky and disfiguring17.
The treatment for venous disease focuses on decreasing ambulatory venous hypertension. Various strategies and new technologies have been evolved to treat all forms of venous disease in a more minimal way.
As endovenous techniques were evolving the traditional surgical therapy has been replaced with minimally invasive methods. These techniques include thermal ablation by laser or radiofrequency and non-thermal ablation by foam sclerotherapy or mechano-chemical obliteration of the insufficient venous trunks. Because of the results of the newer techniques over the standard ones, endovenous techniques are nowadays recommended as first-line treatment for venous trunk reflux, both in the USA and the UK.
In 2013 the National Institute for Health and Care Excellence (NICE) guideline on diagnosis and management of varicose veins that were updated in March 2018, recommends thermal techniques as the first option for the treatment of insufficient veins, foam and liquid sclerotherapy as the second, and open surgery only if the previous methods are unsuitable 18,19.
The goal of ambulatory treatment of CVD is to treat patients without any need for hospitalization, not even for a few hours. The aim is to confine patient’s stay “in hospital” just as long as it is the duration of the procedure, in the same way as a visit to a dentist. In our study we reported patients that were treated on a totally outpatient basis.
We’ve chosen endovenous application of n-butyl cyanoacrylate glue for the closure of the incompetent GSV and small saphenous vein (SSV). All endovenous methods have their pros and cons but in regard with the ambulatory concept, we think that the use of cyanoacrylate glue closure offers more advantages compared to other endovenous modalities. A great advantage is that it does not require perivenous tumescent anaesthesia. The application of tumescent anaesthesia causes some pain and disturbance to the patient, as well as post-operative annoyance and bruising20,21. Moreover, tumescent anaesthesia is time consuming adding anxiety to the patient. The need of tumescent anaesthesia is the reason why in many centers the thermal ablation treatment is used under mild sedation or even under general anaesthesia, so the patient can’t leave immediately after the end of the procedure.
The axial ablation can be combined with superficial phlebectomy in a single setting or in two stages. A debate still exists as to whether the two procedures should be performed simultaneously or in a staged fashion 22,23. In our study, per protocol, we didn’t treat the varicose veins during the initial procedure. but we let them shrink without reflux supply and treated them only if they were visible after three months. The rationale behind this decision was firstly to minimize the discomfort of our patients, as all procedures were done under local anaesthesia, and secondly to treat fewer varicose veins if needed, cause most of them could have been reduced in size and number, without the reflux- derived supply. This hypothesis proved to be true as the appearance of varicose veins improved in 96% of the cases. Thirty-three patients (33%) presented complete obliteration of varicose veins, while 63 patients (63%) showed significant improvementof the appearance of varicose veins. As a result, only 4 patients (4%) needed complementary treatment.
We evaluated our results regarding effectiveness and safeness. At first, we evaluated anatomical success as indicated by GSV occlusion rate on ultrasound examinations, defined as no segments of patency longer than 3 cm. To evaluate treatments in modern medicine, we cannot only report technical success. This is particularly true when we evaluate treatments for chronic venous disease, where there is a strong socio-economic effect24. Moreover, when we try to evaluate an outpatient method, socioeconomic, QoL, and clinical aspects must be assessed. In our study, to evaluate our results, apart from the technical success, we also reported the clinical outcomes, the relief of symptoms, the improvement of disease severity and the cosmetic results
In literature, researchers have used many assessment tools to evaluate the severity of venous disease and to provide standardized reports on effectiveness. Unfortunately, although many methods for venous outcomes assessments have been in use for many years, currently, there isn’t any universally accepted scoring system to compare the outcomes of venous treatments. On the contrary, there are many different outcome assessment tools available, targeting clinical outcomes or quality of life. In part, this reflects different emphasis within each scoring system. As a result, for accurate assessment of the various venous treatments, a combination of clinical scores with quality of life (QoL) outcome measurements system(s) is needed9,25,26.
In an effort to standardize reporting in CVD research the CEAP (clinical, etiologic, anatomic, pathophysiologic) classification system was proposed in 1995. The CEAP clinical classification for chronic venous disease (CVD) is based on physician-evaluated clinical signs of CVD and since its introduction it has been used in a number of clinical investigations to classify CVD clinical presentation and to measure change in CVD over time27.
The CEAP classification system for chronic venous disease proved very useful to classify stages of venous disease and enabled patient comparison among different centres and stud- ies. The problem with the CEAP is that it categorizes the severity of lower limb venous disease at a single point in time and it is relatively static and insufficient for determining changes in venous disease severity. Increasingly, patient-reported qualiy of life (QOL) is an important component in evaluating outcome, providing important information about the burden of illness and especially for changes in illness severity over time. For chronic conditions such as CVD, assessment of QOL can provide important information regarding burden of illness that may not be adequately captured with traditional physician-based measures of morbidity or mortality 28,29,30.
The VCSS was designed to assess changes in venous disease in response to treatment over time with some components subjectively determined by the patient and assessed by the provider. This system Venous Clinical Severity Score (VCSS) was proposed in 2000 from the American Venous Forum (AVF), Ad Hoc Committee on Venous Outcomes Assessment 10,31,32 .
The VCSS system includes 10 clinical descriptors (pain, varicose veins, venous edema, skin pigmentation, inflammation, induration, number of active ulcers, duration of active ulceration, size of ulcer, and compressive therapy use). Each one is scored from 0 to 3, so changes in response to therapy can be assessed. The VCSS has the advantage of minimal intraobserver and interobserver variability and has gained through time general acceptance and is used widely for clinical and research purposes 10,33 . The VCSS that was introduced by Rutherford, has been used successfully in several studies to evaluate various vein treatments and a revised VCSS has been developed to clarify ambiguities, update terminology, and simplify application of the first version10,33.
In our study, in order to evaluate our clinical results, we used both the CEAP and the VCSS. The CEAP classification system categorizes the severity of lower limb venous disease based on objective clinical findings, where the VCSS assess changes with some components determined subjectively from the patient’s point of view. Of the many different venous severity assessment tools available, it has shown to corresponds reliably with the severity of venous disease 34,35,36 .
Our results showed great clinical improvement, cause all patients improved their rVCSS. The postoperative rVCSS was 2.3 with a mean 66% decrease (mean preoperative rVCSS was 6.8)
As far as technical success is concerned the method was effective cause all target veins were obliterated. Our results were comparable to most studies in the literature where the anatomical success of the method is very high. Comparing the cyanoacrylate closure to other endovenous treatment mo- dalities such as laser ablation and RF ablation, no differences were observed in occlusion rates between the three modalities, although maybe a slight variation exists in favour of cyanoacrylate closure37,38,39,40,41,42,43,44 .
As far as safeness is concerned, the side effects were mild. Moreover, there wasn’t any problem from the early discharge from the operating room. The most common side effect in our study was the well-known post-procedural phlebitis of the treated vein which in our series occurred in 28 patients (28%). This phlebitis, which is somehow or other benign and self-limited, occurs after the second postoperative day and usually lasts less than a week. In most cases when it happens it doesn’t need any medication. In few cases (15%) anti-inflammatory drug (Ibuprofen) was prescribed.
The advantages of the procedure in an outpatient setting are too many: it heightens patient satisfaction and minimizes patient stress. Patients don’t have to stay at the hospital overnight, that is a stressful experience for many individuals. People can continue to work at home and participate in their daily routine. Especially during COVID era, patients worry less about hospital transmission of COVID by being discharged immediately after the procedure and day-of-surgery discharge decreases the risk of hospital transmission, by shortened length of stay and reduced interaction with other patients and hospital personnel. Finally, it decreases hospitalization costs. When overnight hospital stay is avoided, there is less use of hospital facilities, bedding, food, and drugs
CONCLUSION
Outpatient treatment of axial veins insufficiency of the low- er extremities, using cyanoacrylate closure is a safe and ef- ficient method. It offers many advantages because it height- ens patient satisfaction and minimizes patient stress, permits rapid return to normal activities, reduces the risk of hospital transmission of infection diseases, and decreases hospitaliza- tion costs. The side effects are mild, and the early discharge doesn’t seem to add any possible risk.
References
- Gloviczki P, Comerota AJ, Dalsing MC, Eklof BG, Gillespie DL, Gloviczki ML, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg 2011; 53(Suppl): 2S-48S
- Eberhardt RT, Raffetto JD, Chronic venous insufficiency. Circulation 2014; 130: 333-346.
- avies AH. The seriousness of chronic venous disease: A review of real-world evidence. Adv. Ther. 2019; 36: 5-12.
- Raffetto JD , Mannello F. Pathophysiology of chronic venous disease. Int. Angiol. 2014; 33: 212-221
- iWittens C, Davies AH, Bækgaard N, Broholm R, Cavezzi A, Chastanet S, et al. Esvs Guidelines Committee. Editor’s choice-management of chronic venous disease: clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg 2015; 49 (06): 678-737
- Attaran R. Latest innovations in the treatment of venous disease. J Clin Med 2018; 7(04): 77
- avlović MD, Schuller-Petrović S. Endovascular tech- niques for the treatment of chronic insufficiency of the lower limb’s superficial venous system. Rev Vasc Med 2014; 2(04): 107-117
- Alun H Davis The Seriousness of Chronic Venous Disease: A Review of Real-World Evidence Review Adv Ther 2019 Mar;36(Suppl 1):5-12.
- Steven Elias Minimally invasive vein surgery: latest options for vein disease Mt Sinai J Med 77:270-278, 2010
- asquez MA, Munschauer CE. Venous clinical severity score and quality-of-life assessment tools: application to vein practice. Phlebology 2008; 23(06): 259-27
- Major R.H. A History of Medicine. Blackwell, Oxford1954
- ones W.H.S. Hippocrates with an English translation. William Heinemann, London1923
- Muller R. Interview with Dr. Robert Muller. Father of modern dayambulatory phlebectomy. Interview by Jose A. Olivencia. Dermatol Surg 1998;24(10):1147-1150
- Muller R. [Treatment of varicose veins by ambulatory phlebec tomy]. Phlebologie 1966;19(04):277-279
- Hampton Andrews, Robert G. Dixon Ambulatory Phlebectomy and Sclerotherapy as Tools for the Treatment of Varicose Veins and Telangiectasias Semin Intervent Radiol. 2021 Jun; 38(2): 160-166.
- Jephta van den Bremer Frans L. Moll Historical overview of varicose vein surgery annals of vasc surg GENERAL REVIEW| VOLUME 24, ISSUE 3, P426-432, APRIL 01, 2010
- Lawaetz M, Serup J, Lawaetz B, Bjoern L, Blemings A, Eklof B, et al. Comparison of endovenous ablation techniques, foam sclerotherapy and surgical stripping for great saphenous varicose veins. Extended 5-year follow-up of a RCT. Int. Angiol. 2017; 36: 281-288.
- Marsden G, Perry MC, Kelly K, Davies AH. Guideline Development Group. NICE guidelines on the management of varicose veins. BMJ 2013; 347: f4279.
- Varicose veins: diagnosis and management (Clinical Guideline 168). National Institute for Health and Care Excellence; 2013 (Updated March 2018). Available at: https://www.nice.org.-uk/guidance/cg168.
- Almeida JI, Kaufman J, Göckeritz O, Chopra P, Evans MT, Hoheim DF, et al. Radiofrequency endovenous Closure- FAST versus laser ablation for the treatment of great saphenous reflux: a multicenter, single-blinded, randomized study (RECOVERY study). J Vasc Interv Radiol 2009; 20: 752-9
- Proebstle TM, Vago B, Alm J, Göckeritz O, Lebard C, Pichot O. Treatment of the incompetent great saphenous vein by endovenous radiofrequency powered segmental thermal ablation: first clinical experience. J Vasc Surg 2008; 47: 151-6
- Lane TRA, Kelleher D, Shepherd AC, Franklin IJ, Davies AH. Ambulatory varicosity avulsion later or synchronized (AVULS): a randomized clinical trial. Ann Surg 2015;261(04):654-661
- ager ES, Ozvath KJ, Dillavou ED. Evidence summary of combined saphenous ablation and treatment of varicosities versus staged phlebectomy. J Vasc Surg Venous Lymphat Disord 2017;5(01):134-137
- Nicolaides A, Kakkos S, Baekgaard N, et al. Management of chronic venous disorders of the lower limbs. Guidelines according to scientific evidence. Int Angiol 2018;37:181- 254
- Zhoupeng Wu, Yukui Ma A narrative review of the quality of life scales specific for chronic venous diseases Medicine (Baltimore). 2021 May 21; 100(20): e25921
- Susan R. Kahn, Cyr E. M’lan, Donna L. Lamping, Xavier Kurz, Anick Be´rard, Lucien A. Abenhaim, et al for the VEINES Study Group Relationship between clinical classification of chronic venous disease and patient-reported quality of life: Results from an international cohort study J Vasc Surg 2004;39:823-8
- Donna L Lamping , Sara Schroter, Xavier Kurz, Susan R Kahn, Lucien Abenhaim Evaluating outcomes in chronic venous disorders of the leg: development of a scientifically rigorous, patient-reported measure of symptoms and quality of life. J Vasc Surg 2003;37:4
- Hamdan A. Management of varicose veins and venous insufficiency. JAMA 2012;308(24):2612-2621
- Eklöf B, Rutherford RB, Bergan JJ, Carpentier PH, Gloviczki P, Kistner RL, et al. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg 2004;40:1248-52
- Porter JM, Moneta GL. and an international consen- sus committee on chronic venous disease. Reporting standards in venous disease: an update. J Vasc Surg 1995;21:635-45.
- klof B, Perrin M, Delis KT, Rutherford RB, Gloviczki P Updated terminology of chronic venous disorders: the VEIN-TERM transatlantic interdisciplinary consensus document. J Vasc Surg 2009; 49:498-501
- Rutherford RB, Padberg FT, Comerota AJ, Kistner RL, Meissner MH, Moneta GL. Venous severity scoring: an adjunct to venous outcome assessment. J Vasc Surg 2000;31:1307-12
- Meissner MH, Natiello C, Nicholls SC. Performance characteristics of the venous clinical severity score. J Vasc Surg 2002;36:889-95.
- Vasquez MA, Rabe E, McLafferty RB Shortell CK, Marston WA, Gillespie D, et al. Revision of the venous clinical severity score: venous outcomes consensus statement: Special communication of the American Venous Forum Ad Hoc Outcomes Working Group. J Vasc Surg 2010;52:1387-96
- Marc A. Passman, Robert B. McLafferty, Michelle F. Lentz, Shardul B. Nagre, Mark D. Iafrati, W. Todd Bohannon et al Validation of Venous Clinical Severity Score (VCSS) with other venous severity assessment tools from the American Venous Forum, National Venous Screening Program J Vasc Surg 2011;54:2S-9S
- Kakkos SK, Rivera MA, Matsagas MI, Lazarides MK, Robless P, Belcaro G, et al. Validation of the new venous severity scoring system in varicose vein surgery. J Vasc Surg 2003;38:224-8.
- Vasquez MA, Wang J, Mahathanaruk M, Buczkowski G, Sprehe E, Dosluoglu HH, et al. The utility of the Venous Clinical Severity Score in 682 limbs treated by radiofrequency saphenous vein ablation. J Vasc Surg 2007;45:1008-14.
- Bozkurt AK, Yılmaz MF. A prospective comparison of a new cyanoacrylate glue and laser ablation for the treament of venous insufficiency. Phlebology 2016; 31(Suppl 1): 106-113
- Morrison N, Gibson K, Vasquez M, Weiss R, Cher D, Madsen et al. VeClose trial 12-month outcomes of cyanoacrylate closure versus radiofrequency ablation for incompetent great saphenous veins. J Vasc Surg Venous Lymphat Disord 2017;5(03): 321-330
- Park I. Initial outcomes of cyanoacrylate closure, Vena- Seal system, for the treatment of the incompetent great and small saphenous veins. Vasc Endovascular Surg 2017; 51(08): 545-549
- Eroglu E, Yasim A. A randomised clinical trial comparing N-butyl cyanoacrylate, radiofrequency ablation and endovenous laser ablation for the treatment of superficial venous incompetence: two year follow up results. Eur J Vasc Endovasc Surg 2018; 56(04): 553-560
- Dimech AP, Cassar K. Efficacy of cyanoacrylate glue ablation of primary truncal varicose veins compared to existing Endovenous Techniques: A Systematic Review of the Literature. Surg J (N Y) 2020; 6(2): e77-e86
- Eroglu E, Yasim A, Ari M, Ekerbicer H, Kocarslan A, Kabalci M et al. Mid-term results in the treatment of varicose veins with N-butyl cyanoacrylate. Phlebology 2017; 32 (10): 665-669
- Yang GK, Parapini M, Gagnon J, Chen JC. Comparison of cyanoacrylate embolization and radiofrequency ablation for the treatment of varicose veins. Phlebology 2019; 34(04): 278-283
- Koramaz İ, El Kılıç H, Gökalp F, Bitargil M, Bektaş N, Engin E, et al. Ablation of the great saphenous vein with nontumescent n-butyl cyanoacrylate versus endovenous laser therapy. J Vasc Surg Venous Lymphat Disord 2017; 5(02): 210-215



{kind=link}
{kind=link}
{kind=link}