

The ‘hook-sign’ in the Median Arcuate Ligament Syndrome
| Available Online: | September, 2023 |
| Page: | 115-116 |
Author for correspondence:
Spyros Papadoulas
Department of Vascular Surgery, University of Patras Medical School, Patras, Greece
E-mail: spyros.papadoulas@gmail.com
ISSN 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications
All rights reserved. https://www.heljves.com
Full Text
Images
Full Text
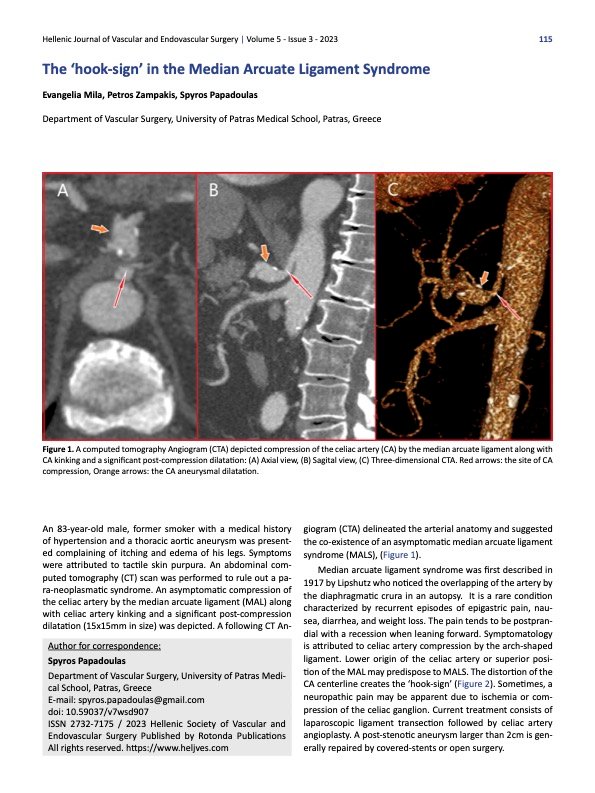
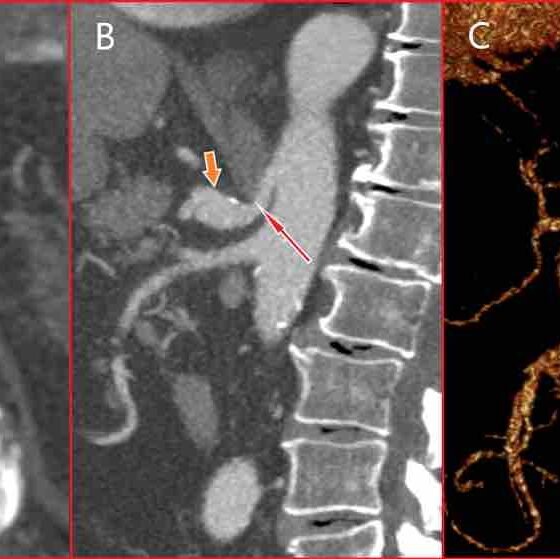
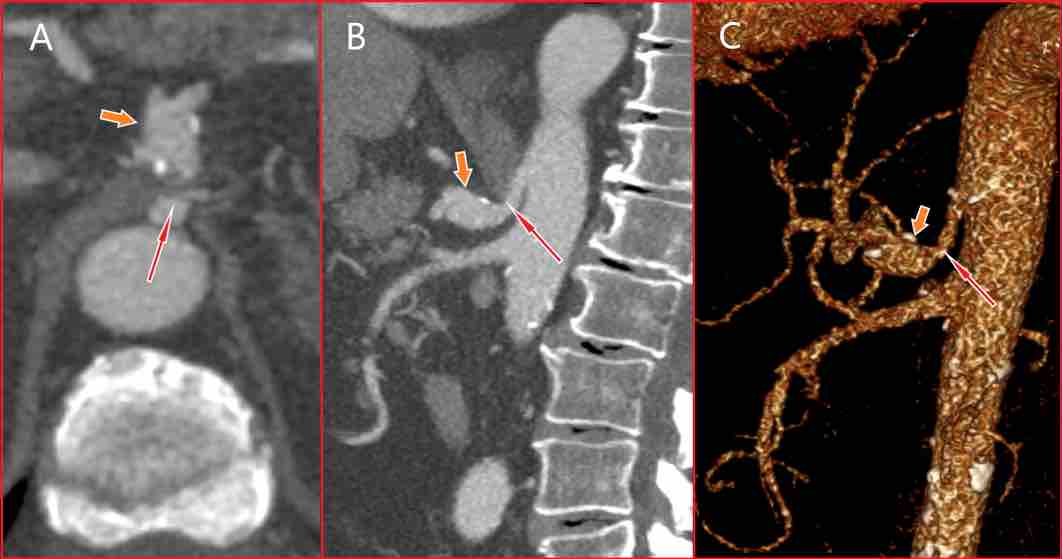
Figure 1. A computed tomography Angiogram (CTA) depicted compression of the celiac artery (CA) by the median arcuate ligament along with CA kinking and a significant post-compression dilatation: (A) Axial view, (B) Sagital view, (C) Three-dimensional CTA. Red arrows: the site of CA compression, Orange arrows: the CA aneurysmal dilatation.
An 83-year-old male, former smoker with a medical history of hypertension and a thoracic aortic aneurysm was presented complaining of itching and edema of his legs. Symptoms were attributed to tactile skin purpura. An abdominal computed tomography (CT) scan was performed to rule out a para-neoplasmatic syndrome. An asymptomatic compression of the celiac artery by the median arcuate ligament (MAL) along with celiac artery kinking and a significant post-compression dilatation (15x15mm in size) was depicted. A following CT Angiogram (CTA) delineated the arterial anatomy and suggested the co-existence of an asymptomatic median arcuate ligament syndrome (MALS), (Figure 1).
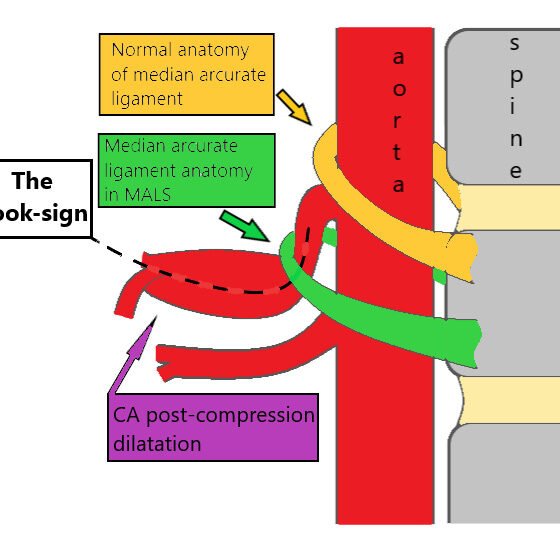
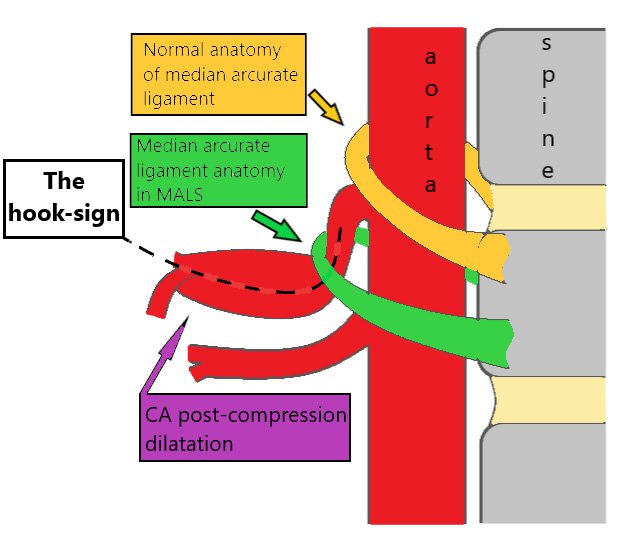
Median arcuate ligament syndrome was first described in 1917 by Lipshutz who noticed the overlapping of the artery by the diaphragmatic crura in an autopsy. It is a rare condition characterized by recurrent episodes of epigastric pain, nausea, diarrhea, and weight loss. The pain tends to be postprandial with a recession when leaning forward. Symptomatology is attributed to celiac artery compression by the arch-shaped ligament. Lower origin of the celiac artery or superior position of the MAL may predispose to MALS. The distortion of the CA centerline creates the ‘hook-sign’ (Figure 2). Sometimes, a neuropathic pain may be apparent due to ischemia or compression of the celiac ganglion. Current treatment consists of laparoscopic ligament transection followed by celiac artery angioplasty. A post-stenotic aneurysm larger than 2cm is generally repaired by covered-stents or open surgery.
{kind=link}
{kind=link}