

Artificial Intelligence and e-Learning will shape the future of vascular surgical training
| Available Online: | October, 2023 |
| Page: | 117-119 |
Author for correspondence:
Nikolaos Patelis
Metropolitan General, 264 Mesogeion Avenue, Cholargos – Athens, Greece
E-mail: patelisn@gmail.com
doi: 10.59037/djr4hv48
ISSN 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Full Text
References
Images
Full Text
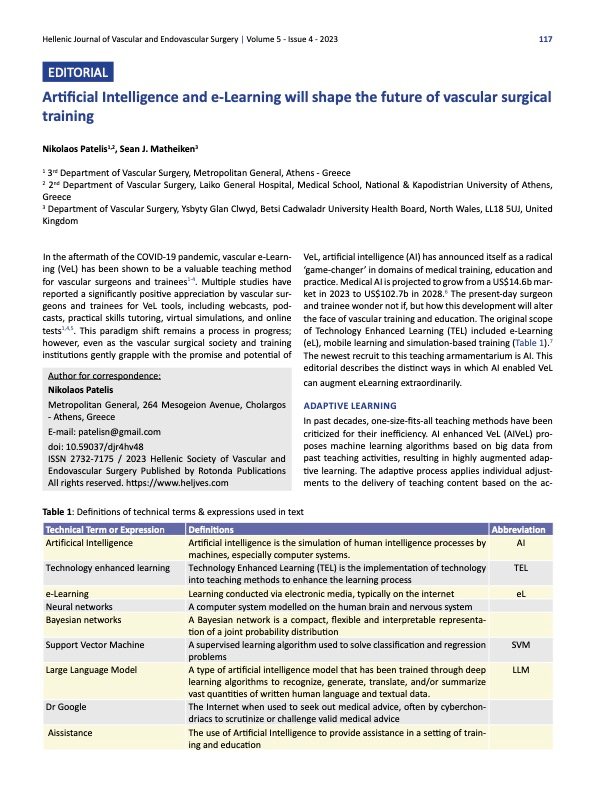
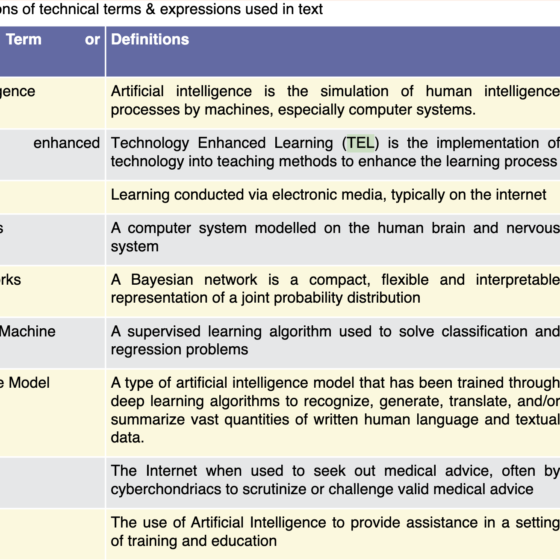
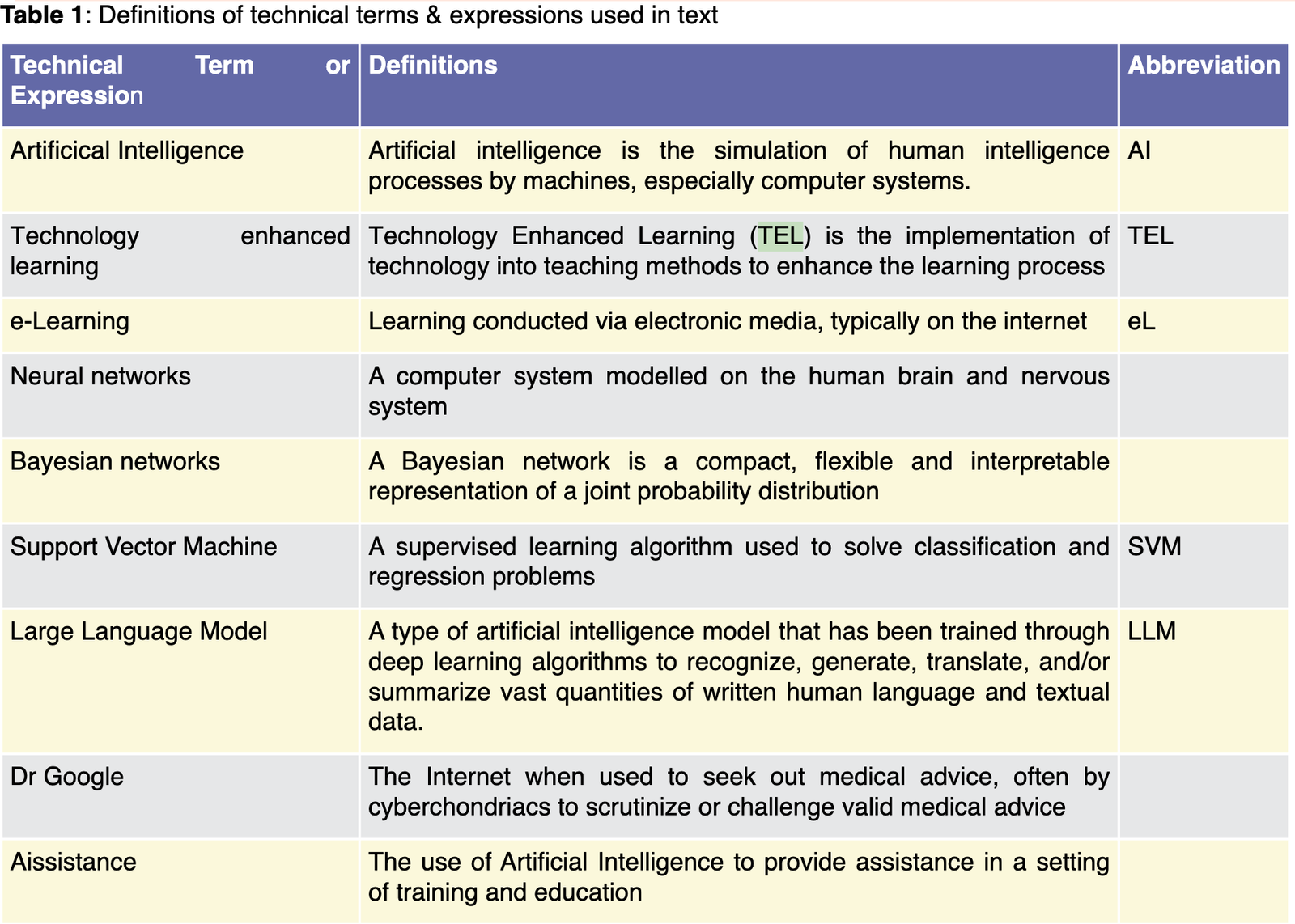
In the aftermath of the COVID-19 pandemic, vascular e-Learning (VeL) has been shown to be a valuable teaching method for vascular surgeons and trainees1-4. Multiple studies have reported a significantly positive appreciation by vascular surgeons and trainees for VeL tools, including webcasts, podcasts, practical skills tutoring, virtual simulations, and online tests1,4,5. This paradigm shift remains a process in progress; however, even as the vascular surgical society and training institutions gently grapple with the promise and potential of VeL, artificial intelligence (AI) has announced itself as a radical ‘game-changer’ in domains of medical training, education and practice. Medical AI is projected to grow from a US$14.6b market in 2023 to US$102.7b in 2028.6 The present-day surgeon and trainee wonder not if, but how this development will alter the face of vascular training and education. The original scope of Technology Enhanced Learning (TEL) included e-Learning (eL), mobile learning and simulation-based training (Table 1).7 The newest recruit to this teaching armamentarium is AI. This editorial describes the distinct ways in which AI enabled VeL can augment eLearning extraordinarily.
ADAPTIVE LEARNING
In past decades, one-size-fits-all teaching methods have been criticized for their inefficiency. AI enhanced VeL (AIVeL) proposes machine learning algorithms based on big data from past teaching activities, resulting in highly augmented adaptive learning. The adaptive process applies individual adjustments to the delivery of teaching content based on the acceptance that learners have diverse backgrounds, learning preferences and cognitive abilities. In the realm of conventional e-learning, such refinement is limited to the incorporation of a degree of ‘program-and-platform-limited’ reactivity into online educational activities. AI supported augmentation of eL matter can utilise AI algorithms to scrutinise learners’ active and legacy interactions with the learning platform in real time. Leveraging this analysis, the system adjusts both the content and presentation of e-Learning modules to provide an individualised course targeting the desired learning outcomes (LOs). Assessing the actual grasp of pertinent knowledge or skills offered online can serve as a gauge for the effectiveness of e-Learning itself. e-Learning environments ought to be flexible enough to facilitate a range of productive activities, recognizing this acquisition as a constructive process that can manifest in diverse forms of learning engagement. Assistance from automated bots in an AI assisted eL environment would further bolster the learning experience. Examples of this vary in complexity; direct feedback to an incorrect response, incremental hints towards the correct response and technical tutoring to address targets of improvement. The application of AI analysis to composite learner responses and incorporation of these findings to derive a customised user algorithm that also subsumes influence from big data analysis will result in unparalled adaptability of eL material. The powerful tailoring of both the quality and quantum of ‘AIssistance’ made possible in this way will facilitate achievement of intended LOs by each individual user in the most efficient manner possible. Such AIVeL-based adaptive learning has immense potential to overcome the high dropout rates and low engagement previously described with e-Learning, further improving collective outcomes.
The results of adaptive AIVeL very significantly depend on the data harvest and analysis tool (e.g. neural networks, Bayesian networks or Support Vector Machines), as well as on the type of e-Learning used (e.g. micro-adaptive, macro-adaptive, linear). Each combination of an AI tool and an e Learning type could alter significantly the output of the AIVeL system and either lead to positive or negative user experience.
LARGE LANGUAGE MODELS
Establishment of AIVeL as a training technology is likely, as with most new modalities, to take initial root in well-funded academic environments. Beyond this anticipated pilot phase, the ability of advanced AI language capabilities to offer VeL content to diverse groups in their native languages on the fly, without prior translation, will facilitate exponential scalability of AIVeL to the global market. A further benefit AIVeL could offer vascular education is the use of natural language algorithms for the grading and assessment of open text from content such as dissertations. Modern day AI models for such tasks are highly sensitive to plagiarism and can distinguish discrepancies of writing style to detect fraud.
At the same time, Large Language Models (LLMs) possess an ever-expanding capacity to generate text indistinguishable from human writing. The ability of LLMs to construct coherent and contextually appropriate content across various domains will inevitably blur the lines between genuine human-generated work and AI-generated content in all fields including vascular surgery. The misrecognition of AI-authored e-Learning materials as human-created content has real potential to significantly exacerbate the already recognised “Dr Google” phenomenon, wherein users accept unaccredited medical material as per se correct. Unpublished research by ChatAortaAI has already identified variables that determine the results of LLMs – these include the particular language used, the available bid data in that language on a given subject and the phrasing of the ‘input request’ by the user.8 The AI-generated answer to a clinical question therefore depends on the language the user uses, the size of available big data in this language and finally the wording of the question.
It is important to appreciate the above practical challenges of accurate attribution of authorship posed by the advent of AIVeL. The unearthing of flawed or fraudulent AI-authored e-Learning materials will pose a further conundrum – if the best tool for ferreting out the ‘bad apple’ AIVeL output is, by definition, another AI algorithm, will this represent a situation of ‘marking one’s own homework’? These are fertile grounds for technical and ethical debate.
SIMULATION AND LIVE ASSISTANCE
The use of simulation in vascular surgery is well established and positive results have already been published.9 The use of AIVeL will substantially augment the level of detail and degree of finesse that can be enabled during a simulated ‘pre-operative training run’ on the specific patient’s own anatomy in both open or endovascular settings. In addition, AI can enhance actual operative procedures by providing real-time guidance and assistance to vascular surgeons. An example of such an application would be AI mapping of advanced imaging and pre-operative road-mapping of the intended operative journey in a manner similar to the use of fusion registration of CT data during fenestrated EVARs. The ability of AI AI algorithms to identify imminent complications based on the extent of deviation of the actual operative steps from the preoperative ‘intended path’ within the context of individual anatomy and anomalies will enable use of such a technological safeguard in a way hitherto impossible during open surgery. AI augmented reality overlays during surgery can “AIssist” accurate incisions, define approaches to tissue too scarred for the human eye to distinguish planes and flag up ‘rogue bites’ falling outside predefined parameters of adequacy during an anastomosis. The potential of such capabilities to reduce human error and enhance overall precision is indescribable. Additionally, AI algorithms can continuously analyze data from various sources (e.g. monitors, angiograms), predicting potential complications and providing immediate recommendations, ultimately improving patient outcomes and fostering a safer surgical environment. All the above could be of great significance to young vascular specialists as well as to trainees.
The potential of AIVeL comes into its own further still in the practical domain. Examples of such tutoring vary widely in complexity; a few would be direct feedback to an incorrect response, incremental hints towards the correct response and technical tutoring to address targets of improvement in learning techniques. Such haptic and iterative feedback already exists in the endovascular simulator based domain.10 The superadded value conferred by AIVeL would fall into two broad categories. The first is the ability to present a multitude of potential ‘technical’ permutations derived from big data, filtered to the learner’s choice. The user may choose to train on the most common patterns encountered in clinical practice, or to challenge themselves on the most complex presentations, as just two examples of preference. The second benefit is the unique capability of AI to provide analytical feedback in response to each training ‘run’ to a degree of finesse and depth that a simulator cannot accomplish and which most human trainers could not sustain consistently. Both these unique advantages would derive from AI interpretation of prior responses from the individual student and algorithms derived from big data analysis.
IMAGE GENERATORS
AI can create graphics and animations in vascular anatomy, vascular physiology and haemodynamics based on reality. The accuracy level achievable by such image generators is projected to improve exponentially over this decade. AIVeL depictions that are liberated from the inaccuracies that blight representations created as a likeness would provide a powerful tool for learning; they would also offer unparalleled potential for reversing the supply demand imbalance in many healthcare sectors globally while – paradoxically – strengthening rather than weakening the credentialling of skill sets of ‘new’ operators. The favourable impact such training and practice models would proffer to patient safety profiles would help recruit support for AIVeL from regulatory and governance bodies.
CONCLUSION
The era of AIVeL appears to be upon us. There is much to deliberate about its potentials and pitfalls. It may be more pragmatic to engage actively with the practicalities and safeguards of implementing AIVeL, rather than permitting that process to progress without our involvement.
References
- Patelis N, Bisdas T, Jing Z, et al. Vascular e-Learning during the COVID-19 pandemic: the EL-COVID survey. Ann Vasc Surg. 2021.
- Dickinson KJ, Caldwell KE, Graviss EA, et al. Assessing learner engagement with virtual educational events: Development of the Virtual In-Class Engagement Measure (VIEM). Am J Surg. 2021;222(6):1044-1049.
- Fabiani MA, Gonzalez-Urquijo M, Cassagne G, et al. Thirty-three vascular residency programs among 13 countries joining forces to improve surgical education in times of COVID-19: A survey-based assessment. Vascular. 2022;30(1):146-150.
- Jogerst K, Chou E, Tanious A, et al. Virtual Simulation of Intra-operative Decision-Making for Open Abdominal Aortic Aneurysm Repair: A Mixed Methods Analysis. J Surg Educ. 2022;79(4):1043-1054.
- Patelis N, Rielo-Arias F, Bertoglio L, Matheiken SJ, Beard JD. Modular e-learning for a practical skill in vascular surgery. Hellenic J Vasc Endovasc Surg. 2020;2(1):31-34.
- Artificial Intelligence in Healtcare market. 2023; https://www.marketsandmarkets.com/Market-Reports/artificial-intelligence-healthcare-market-54679303.html?gad_source=1&gclid=Cj0KCQjwy4KqBhD0ARIsAEbCt6hzTF-t2FehaJkNH8hidFIfAeBbFkiqfAL_LISBYKLyqZxji3UPXbcaApF0EALw_wcB. Accessed 31/10/2023.
- Patelis N, Matheiken SJ, Beard JD. The challenges of developing distance learning for surgeons. Eur J Vasc Endovasc Surg. 2015;49(3):237-238.
- Think Tank Aorta. 2023; https://www.linkedin.com/company/think-tank-aorta/. Accessed 07/12/2024.
- Haiser A, Aydin A, Kunduzi B, Ahmed K, Dasgupta P. A Systematic Review of Simulation-Based Training in Vascular Surgery. J Surg Res. 2022;279:409-419.
- Hislop SJ, Hsu JH, Narins CR, et al. Simulator assessment of innate endovascular aptitude versus empirically correct performance. J Vasc Surg. 2006;43(1):47-55.
{kind=link}