

Ruptured Degenerative Common Femoral Artery Aneurysm

| Available Online: | April, 2024 |
| Page: | 67-68 |
Author for correspondence:
Emmanouil Barmparessos
Vascular Surgery Department, University Hospital of Patras, Rio, 26 504, Greece
E-mail: mparmpar@ac.upatras.gr
doi: 10.59037/32r6wf96
ISSN 2732-7175 / 2024 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Vascular Surgery Department, University Hospital of Patras, Rio, 26504, Greece
Full Text
References
Images
Full Text
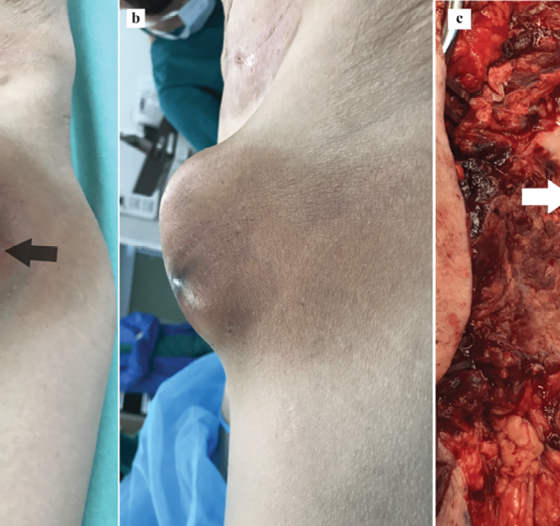
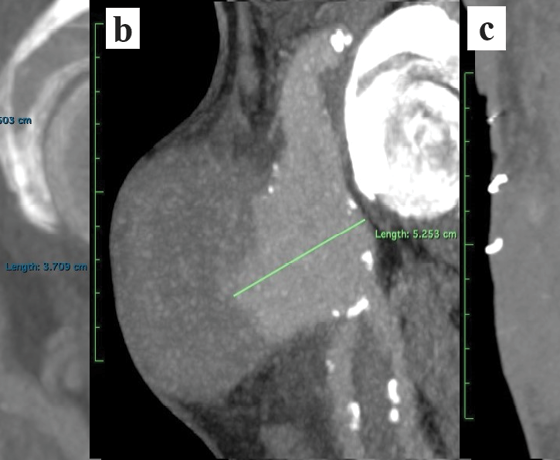
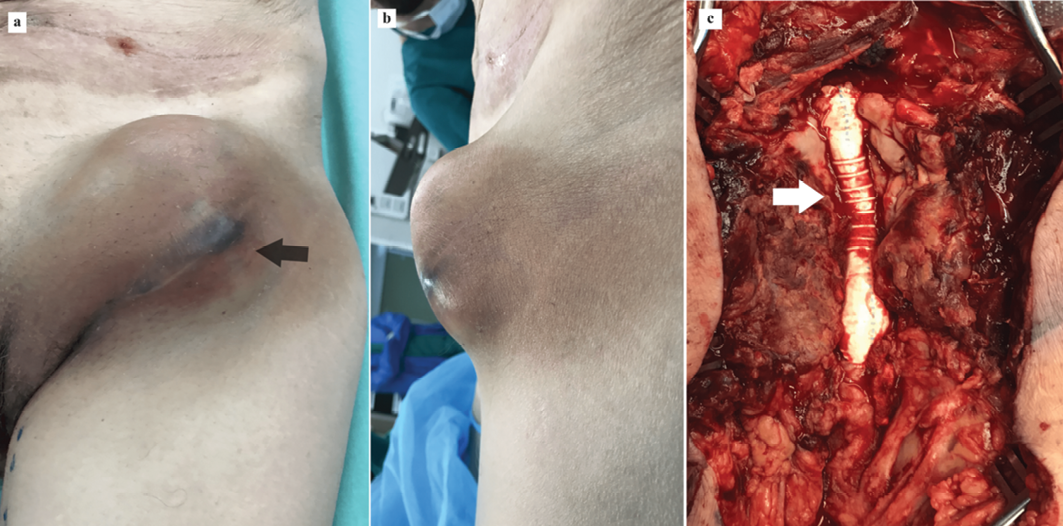
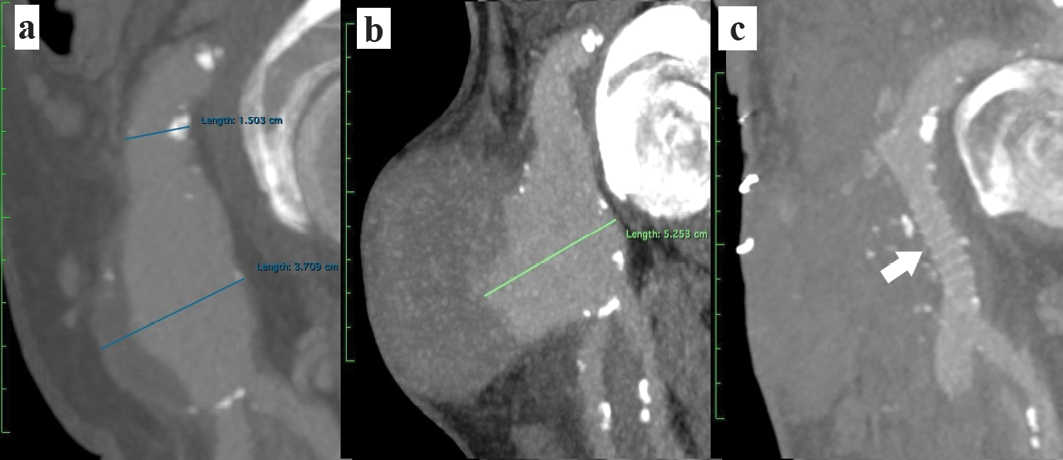
A 75-year-old male patient presented acutely complaining of a painful and increased in size left inguinal mass. Being haemodynamical stable, physical examination revealed a severe palpable inguinal mass where the overlying skin was erythematous with spots of imminent necrosis (Figure 1a and b). He had a history of Endovascular aortic Aneurysm Repair (EVAR) eight years ago on the background of aneurysmatic disease progression following an initial open repair of his abdominal aortic aneurysm seventeen years ago. Urgent Computed Tomography Angiography revealed an isolated ruptured Common Femoral Artery Aneurysm (CFAA) (Figure 2b). Right afterwards, under general anaesthesia proximal control was obtained by exposing, through a longitudinal incision, the very distal left External Iliac Artery (EIA) right above the inguinal ligament and distal control by exposing the proximal superficial femoral artery. Following haematoma and aneurysmatic sac evacuation, back-bleeding from the profunda was halted by inflating a 3Fr Fogarty catheter. Then, arterial reconstruction was succeeded by an 8mm polytetrafluoroethylene graft (Gore Propaten, Flagstaff, AZ, USA) anastomosed proximally to the EIA and distally to the common femoral bifurcation (Figure 1c). Recovery was successful, patient was discharged and returned in three-weeks-time for an endovascular repair of his bilateral type Ib endoleaks. True isolated CFAA is rare with an incidence of five patients per 100,0001. Up to 60% of the cases are asymptomatic and recent data suggest that risk of complications like rupture (6%) or thrombosis (4%) are rare for those smaller than 3.5cm2. Our patient had a CTA a year ago which showed a left CFA measuring 3.7cm but was not picked up (Figure 2a). Clearly our case shows how aneurysmatic disease progresses with time and sets a high suspicion for an underlying connective tissue disease.
Acknowledgements
None
None declared.
References
- Piffaretti G, Mariscalco G, Tozzi M, Rivolta N, Annoni M, Castelli P. Twenty-year experience of femoral artery aneurysms. J Vasc Surg. 2011 May;53(5):1230-6.
- Lawrence PF, Harlander-Locke MP, Oderich GS, Humphries MD, Landry GJ, Ballard JL, et al. The current management of isolated degenerative femoral artery aneurysms is too aggressive for their natural history. J Vasc Surg. 2014 Feb;59(2):343-9
{kind=link}
{kind=link}